Babu Paul, Director BRiQ MSS
- That was the day of Management Review Meeting at a premier fighter aircraft overhaul depot of Indian Air Force. April is the time we do the “post-mortem” after the hectic production year completion.
- Chief of Aircraft (CA) was in his analytical best. He leaned on the back of his revolving chair and started. “Reliability of the Avionic aggregates has gone down drastically. It is evident from the customer
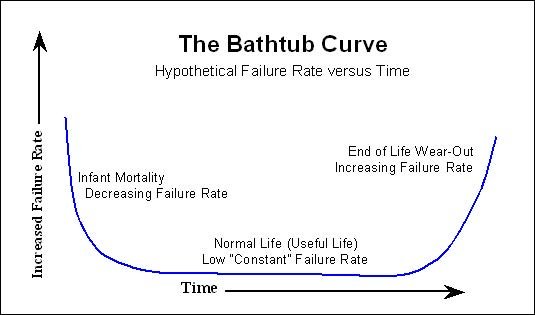
feedback (understand as panic calls from operating squadrons for items) which I keep getting throughout the day. Also, look at your increased Premature Withdrawal Rate (PWR). The Average Service Life (ASL) of many reparable are less than 50% of the To Be Overhauled (TBO) life of 1000 Hrs of flying. We cannot go on like this. Pull up your socks and get to the bottom of this issue. I need a road map in next ten days”. He was in his no nonsense posture. Good sense prevailed, we kept quit and did not give the standard excuses of infant mortality, substandard packing for transportation, extreme weather at operational bases, aging fleet and poor operational and maintenance practices at operating units. - I was working as a Production Engineer(PE) in the Avionics Reparable Servicing Division. My colleague had rich experience in The type aircraft maintenance and overhaul. After CA’s “Moral Lecture (ML)” we came back to the Division and sat down for brain storming. The Quality Circle of the Division was asked to study and propose an Action Plan. We decided that the division should proceed with a Process Improvement Programme through PDCA cycle.
- W.E. Deming the celebrated Quality Guru adapted the Shewhart Cycle into PDCA cycle. A PDCA cycle is used frequently in Quality Management Systems (QMS). PDCA is briefly described in IS/ISO 9001:2008 Standard as follows:
Plan: establish the objectives and processes necessary to deliver results in accordance with customer requirements and the organization’s policies;
Do: implement the processes;
Check: monitor and measure processes and product against policies, objectives and requirements for the product and report the results;
Act: take actions to continually improve process performance.
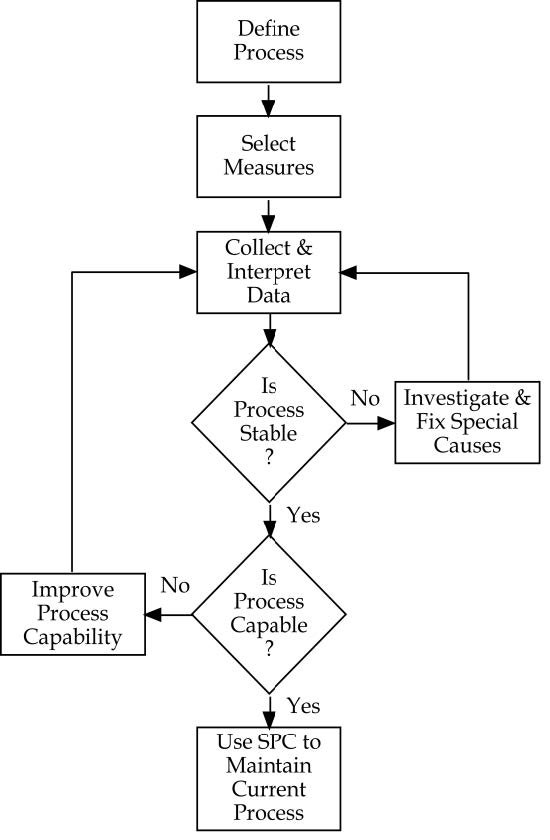
- During each phase of this continual improvement program the Key Result Areas or Objectives have to be defined in advance. The diagram below depicts the KRAs in each phase of PDCA.
- The Process The process of aggregate repair/Overhaul comprises of stages specified in the Work Packages. The avionic reparable (also termed as rotable or aggregate) are send for repair/overhaul on completing the TBO hours to the Avionics Reparable Servicing Division. On receipt, the item undergoes following stages of process during overhaul/repair:

- The Problem The specific problem of failure prior to completion of the assigned useful life after repair/OH for 25 unique lines of avionic reparables of The fleet were at an alarming rate (High Failure Rate Aggregates, HFRA). This was not up to the reputation of the division. Also it amounted to, reducing the fleet serviceability and compromising the operational preparedness of squadrons, extra working hours put in by technicians at BRD/units and loss to exchequer due to additional expenditure on spares, consumables, transportation and time.
- First Cycle of PDCA Following were the stages of first cycle of PDCA:-
(a) Plan Brain storming was conducted by the Quality Circle of the Division. A road map was charted as follows:-
(i) Collect Failure Data of reparable for last five years.
(ii) Collect repair details of all failed repairable.
(iii) Identify the High Failure Rate Aggregates (HFRA) as per the criteria given in Air HQ letter on the topic.
(iv) Prepare Defect Trend Analysis of each of the HFRAs.
(v) Research for Reliability Improvement by eliminating the causes of failure through Reliability and Maintainability (R&M) study for the HFRA.
(b) Do As planned, the Division accomplished the following in Do Phase:-
(i) The failure data of last five years were collected from QA Department.
(ii) Repair data was collected from all production Labs of the Division.
(iii) Aggregates with low Mean Time Between Failure (MTBF) or Average Service Life (ASL) were identified as High Failure Rate Aggregates (HFRA). Few of the identified ones are Flight Data Recorder (FDR), Auto Pilot Computer, Fuel Computer, Helmet Mounted Target Designation System (HMTDS), Limit Control Unit of Engine System, Radar System and V/UHF Radio System.
(iv) Defect Trend Analysis of the HFRAs revealed the following vital few among the trivial many:-
(aa) Failure of OLD Capacitors (14 to 17 years old electrolytic capacitors) amounted to approximately 43% of failure (ageing and value change due to degradation).
(ab) Failure of PCBs due to overheating amounted to 12% of failures. Insufficient cooling was suspected.
(ac) Inaccurate voltage inputs were measured in cases where discrete components of PCBs were fount burnt ( 8% of total failures).
(ad) Remaining failures were either random or not confirmed in the Labs.
(v) The Defect Trend Analysis (DTA), R&M studies and research led to charting a Reliability Improvement Programme for each of the 25 types of reparable. The salient aspects are listed below:-
(aa) OEMs have been upgrading the Radar by replacing the OLD Capacitors with new advanced capacitors.
(ab) Sufficient stock of new capacitors were available in the Division Logistic stores with all ranges of required capacitance and sizes. .
(ac) One to one replacement as per capacitance and sizes for fitment space were proposed by the division and agreed to by Local Technology Committee (LTC) of the depot who oversees modifications. The complex cases were forwarded to Regional Certification Authority for Military Aircraft (RCMA) for approval.
(ad) For few items perforations as cooling vents were put on the body of the metallic cover and adding miniature DC fans were proposed to enhance cooling.
(ae) Voltage tapping changes were possible as multiple output options are given in the OEMn Transformers. This ensured correct voltage levels at PCB inputs.
(c) Check On approval of the Reliability Improvement Programme from LTC the efficacy of the programme was to be checked thoroughly by following the listed steps:-
(i) Two prototype each were prepared with the modifications incorporated.
(ii) Burn through checks by 50 Hrs Lab operation including four Hrs continuous operation per day were performed and all parameters were measured during various instances during the day.
(iii) Reliability Improvement Plan along with test results were put up for clearance for flight trials from Regional Director of RCMA.
(iv) On approval, flight trials for two sorties were carried out.
(v) Items were withdrawn and all parameters were checked for consistency and was found to be within limits.
(d) Act On successful lab checks and flight trials the items were send for field trials for 50 Hrs of operational flying on aircraft. Proto type one each was send to a different operational base to ensure stability in environment conditions. The field units were instructed to return the items to the repair division if successful operation has been accomplished or as soon as a failure occurs. This was fulfilled during 2005-06 for 25 different aggregates and the number of cases of failure occurred in the modified reparable were negligible. The cases of failure were minutely analysed to see the cause of failure to rule out repetitive failure or modification as the reason for the snag. - Second Cycle of PDCA. Following was the sequence of second PDCA:-
(a) Plan On successful first PDCA cycle, the Division embarked on the second cycle. The Plan phase comprised of:-
(i) Planning for provision of spares, components and consumables.
(ii) Formulation of training schedule for technicians after dovetailing the modifications and standardising the Work Packages.
(iii) Survey of repairable held (serviceable and faulty) in field units, Base Logistics and Repair Depot.
(iv) Plan to cater to increased production by extra working hours and pooling of man power.
(b) Do The do phase implemented the actions envisaged in plan phase and the production was staggered to meet the task, field unit demand etc.
(c) Check Regular data analysis (once in a quarter) has been accomplished to check the fleet serviceability and increase in Average Service Life (ASL) and Mean Time Between Failure (MTBF) of each reparable as the % of reparable upgraded were increasing. A positive improvement was recorded as the failure rate reduced by 50% within one year of starting the fleet up gradation programme and 30% of the assets in the fleet were up graded.
(d) Act In the act phase the complete fleet up gradation was to be ensured and the reliability of the up gradation programme evaluated by correlating with the failure data. No unusual spike observed in any case. Steady reduction in failure pattern was observed. - Next Cycles of PDCA The goals of the subsequent PDCA cycles were as follows:-
(a) To evaluate the reliability of modified reparable after three to four years and five to seven years of modification. On an average a reparable is returned to overhaul Division after seven years for overhaul if no failure happens during this period. Parameters of vintage Capacitors, efficiency of DC fans and health of transformers were to be checked.
(b) To find new vital few of freshly identified HFRAs for the quarter by following similar paths as in first and second cycle of PDCA.
(c) If any modified aggregate continues as HFRA, new vital few are to be identified for further improvement. Only one item was coming under this category. - Benefits of PDCA study. The benefits are as follows:-
(a) The approach provided a systematic methodology for process improvement of Reliability Improvement of Avionics Reparable of the aircraft.
(b) Morale and team spirit improved and the team was ready to take up new projects.
(c) Serviceability of fleet increased within two years of starting the project.
(d) Multiple critical demands on a single item was minimal (2 to 3 only). Priority demands reduced by 40%.
(e) By ensuring better serviceability of aircraft at field units with reliable components, the image of the Reparable Servicing Division and Depot was enhanced in the whole of Indian Air Force.
(f) The confidence level of technicians, supervisors and middle managers has improved with this approach and accelerated the process of Lean Manufacture. The PDCA is the step towards Six Sigma as DEMAIC follows the similar philosophy.
(g) The division was awarded Best Quality Circle during the Year for successful initiative. - All is well ! In the Jelebi, Samosa & Chai Party, Chief Production Engineer was proud to call the CA (a new one of course as the Group Captains gets posted out faster in IAF) as a guest and the CA was lavish in praising the good work done by the Avionics Reparable Servicing Division.
(The article was published in Naval Aircraft Quality Assurance Journal)